Are we optimising patient outcomes in frontline multiple myeloma patients?
Outcomes in multiple myeloma have improved in the last 5 to 10 years. However, myeloma remains incurable, and many patients ultimately relapse. The 5-year survival rate is estimated to be 58% in the US.1,2
Historically, 1L non-transplant patients have had worse survival than transplant patients.2
PFS Outcomes by Transplant Status2*
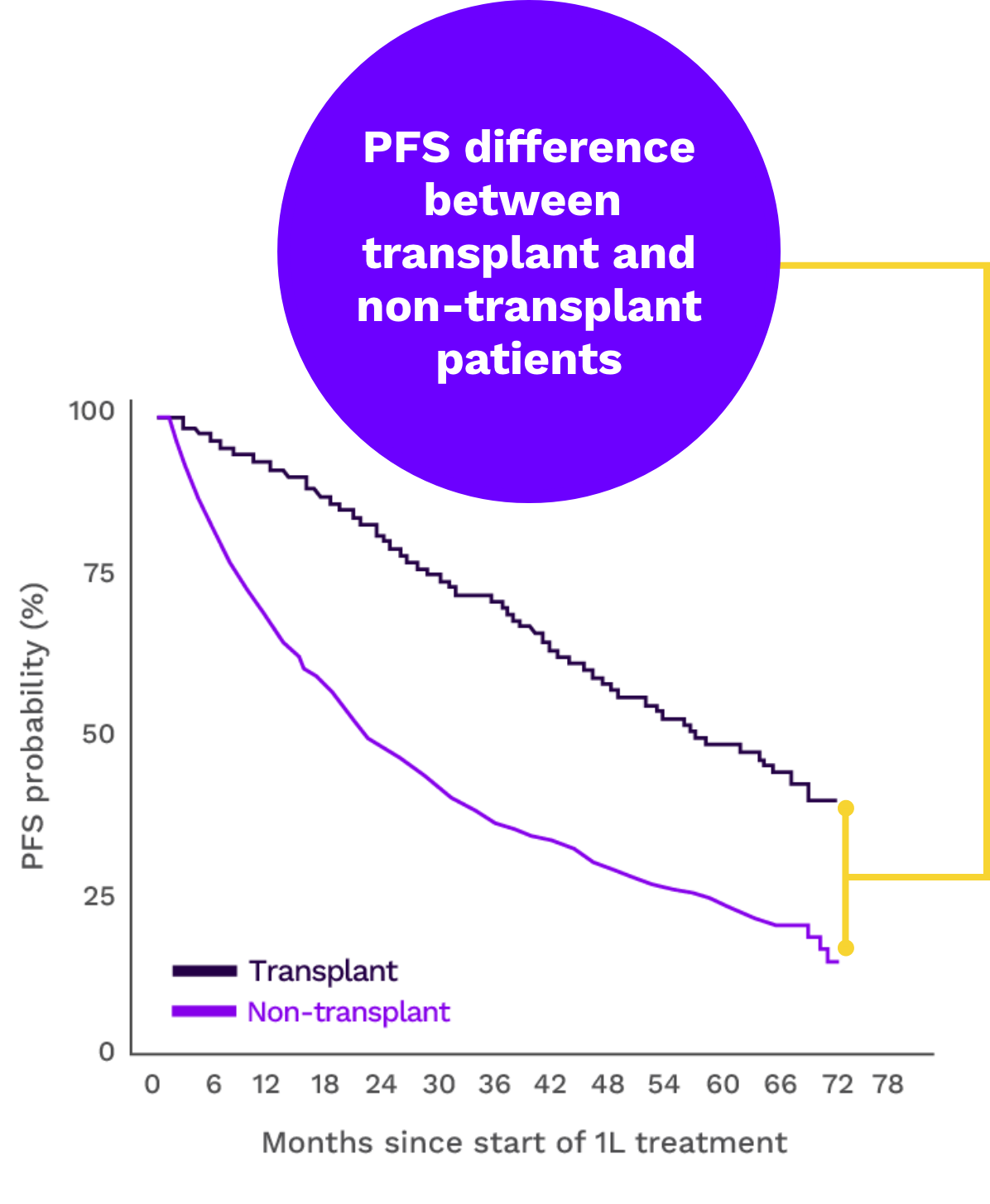
Adapted from Richter J et al. eJHaem. 2023;4(4):984-994. doi:10.1002/jha2.739
Evolving frontline multiple myeloma care is key to improving outcomes. There is a focus on new approaches for non-transplant patients whose prognosis lags behind that of transplant patients3,4
*STUDY DESCRIPTION: A real-world retrospective, observational study of frontline NDMM patients (N=5052) conducted in the US from 1 January 2011 to 31 January 2022.2
Treating to achieve MRD negativity as the ultimate goal in 1L is a potential strategy for optimising outcomes5,6
Maximising depth of response in 1L is vital for early and rapid suppression of clonal heterogeneity because myeloma subclones can evolve into a more challenging disease over time.5,7
Currently, MRD- is the most sensitive measure of depth of response. Recent meta-analyses indicate that MRD- patients tend to experience longer PFS and OS than those who remain MRD+.5,7
Two recent studies, involving 722 US and 700 EU patients, analysed PFS outcomes in newly diagnosed patients treated with either systemic therapy plus transplant or systemic therapy alone. The results were stratified by treatment modality (transplant vs non-transplant) and MRD status (MRD- vs MRD+).3,5,8
PFS Outcomes by Transplant and MRD negativity Status5†

Adapted from Perrot A et al. Blood. 2018;132(3):2456-2464.
Studies indicate that non-transplant patients who achieve MRD negativity may have outcomes comparable to those receiving a transplant4,5
†STUDY DESCRIPTION: 700 newly diagnosed transplant-eligible myeloma patients were randomised to receive different therapies; MRD status was evaluated at the 12-month mark.5
1L=first line; MRD=minimal residual disease; MRD-=minimal residual disease negative/negativity; MRD+= minimal residual disease positive/positivity; NDMM=newly diagnosed multiple myeloma; OS=overall survival; PFS=progression-free survival.
REFERENCES: 1. Nandakumar B, Kapoor P, Binder M. Continued improvement in survival of patients with newly diagnosed multiple myeloma (MM). Blood. 2020:136(Supplement 1):30-31. 2. Richter J, Pan D, Salinardi T, Rice MS. Real-world multiple myeloma front-line treatment and outcomes by transplant in the United States. eJHaem. 2023;4(4):984-994. doi:10.1002/jha2.739 3. Richardson PG, Jacobus SJ, Weller EA, et al; DETERMINATION Investigators. Triplet therapy, transplantation, and maintenance until progression in myeloma. N Engl J Med. 2022;387(2):132-147. doi:10.1056/NEJMoa2204925 4. Mian H, Reece D, Masih-Khan E, et al. Survival and outcomes of newly diagnosed multiple myeloma patients stratified by transplant status 2007-2018: retrospective analysis from the Canadian Myeloma Research Group Database. Clin Lymphoma Myeloma Leuk. 2022;22(8):608-617. doi:10.1016/j.clml.2022.03.002 5. Perrot A, Lauwers-Cances V, Corre J, et al. Minimal residual disease negativity using deep sequencing is a major prognostic factor in multiple myeloma. Blood. 2018;132(23):2456-2464. doi:10.1182/blood-2018-06-858613 6. Burgos L, Puig N, Cedena MT, Mateos MV, Lahuerta JJ, Paiva B, San-Miguel JF. Measurable residual disease in multiple myeloma: ready for clinical practice? J Hematol Oncol. 2020;13(1):82. doi:10.1186/s13045-020-00911-4 7. Suzuki K, Nishiwaki K, Yano S. Treatment strategies considering micro-environment and clonal evolution in multiple myeloma. Cancers (Basel). 2021;13(2):215. doi:10.3390/cancers13020215 8. Supplement to: Richardson PG, Jacobus SJ, Weller EA, et al; DETERMINATION Investigators. Triplet therapy, transplantation, and maintenance until progression in myeloma. N Engl J Med. 2022;387(2):132-147. doi:10.1056/NEJMoa2204925